
Blog

What is Ketamine?
Ketamine (ketamine hydrochloride) is a dissociative anesthetic with some hallucinogenic effects, meaning it distorts perceptions of sight and sound and makes the user feel disconnected from their environment and any pain.1 It has one-tenth the potency of PCP, and its original use is as an injectable, short-acting anesthetic for use in humans and animals.5 Ketamine can induce a state of sedation (feeling calm and relaxed), immobility, relief from pain, and amnesia (no memory of events while under the influence of the drug).1 It can be used for the induction (the transition from an awake to an anaesthe-tized state) of general anesthesia as a pre-anesthetic to other general anesthetic agents.2
Potential Therapeutic Use
Studies from Yale research labs showed that ketamine triggers “glutamate production,” which can prompt the brain to form new neural connections. This makes the brain more adaptable and able to create new pathways, giving patients the opportunity to “develop more positive thoughts and behaviors.” This was an effect that had not been seen before, even with traditional antidepressants.4 For the last two decades, researchers at Yale have led ketamine research by experimenting with using small doses of ketamine delivered intravenously in controlled clinical settings for patients with severe depression who have not improved with standard antidepressant treatments. In several studies, more than half of participants (who felt other antidepressant medications were ineffective) showed a significant decrease in depression symptoms after just 24 hours. The study states that ketamine “needs to be part of a more comprehensive treatment plan.”4 Studies are continuing to explore the possibilities of ketamine in therapeutic settings. It is not unlikely to assume that as ketamine gets clinically used, it will unfortunately also be under threat of being abused or misused.
Ketamine Misuse
Much like its intended use, ketamine can be misused recreationally for its ability to produce dissociative sensations and hallucinations. In 2022, the American Addiction Centers reported that nonmedical misuse is relatively low, with 0.7% of the U.S. population using it illegally.6
Since ketamine can be used in powdered form, it has been known to be snorted as a “party drug” at festivals or rave events.3 The street name for ketamine is “K” or “Special K.”
Ketamine has also been used to facilitate sexual assault because of its hallucinogenic effects known to make the user feel disconnected from their surroundings. A number of individuals have abused this drug or have been instrumental in others using this drug as a “date-rape” drug.1
Recreational use of ketamine can result in a number of internal complications including:
- gastrointestinal issues;
- depression;
- respiratory problems and;
- amnesia
Serious debilitating urinary tract symptoms are also seen frequently in those individuals who abuse ketamine.3 A study on ketamine in the National Institutes of Health predicts that ketamine toxicity and addiction “pose significant risks to a small segment of the population, and given increasing utilization, the prevalence of these phenomena is expected to increase.5” As ketamine use increases both recreationally and clinically, it will continue to be a substance worth testing for.
USDTL Testing
As an innovative leader offering alcohol and other drug testing, we understand the importance of being able to test when it is most feasible for your organization. We offer extended panel testing for ketamine in alternative specimens including hair, nail, urine, and umbilical cord tissue.
References:
- 3: https://clinmedjournals.org/articles/ijda/international-journal-of-depression-and-anxiety-ijda-1-006.php?jid=ijda
- 4: https://www.yalemedicine.org/news/ketamine-depression
- 5: https://www.ncbi.nlm.nih.gov/books/NBK541087/
- 6: https://americanaddictioncenters.org/ketamine-abuse

ToxTime: Choose the Best Test – An Overview of Advanced Alcohol & Other Drug Testing Options
Please join us for ToxTime with Guida Brown, Guided by Guida, discussion over detection windows for a variety of drug and alcohol tests.
Description:
Choosing the best test is determined by what information is sought. Testing of urine, blood, hair, or nails, among other substances, each serves a purpose, but the right test is needed for the results to be useful to anyone. During this free ToxTime presentation, Guida Brown of Guided by Guida will discuss detection windows for a variety of tests and how the results garnered can best be used. A recording of the presentation and a certificate of attendance will be available 24-48 hours after the completion of the webinar.
Speaker:
Guida Brown earned a bachelor’s degree in Journalism from Marquette University and a master’s degree in Management from Cardinal Stritch University; Guida Brown made the nonprofit sector in Kenosha County her career. She was the Executive Director of the Hope Council on Alcohol & Other Drug Abuse, Inc., for over 13 years, resigning from that position in June 2022. Prior to her tenure at the Hope Council, she worked as the Director of Human Resources and Training at AM Community Credit Union and Executive Director at Women and Children’s Horizons. She is the Principal for Guided By Guida, as well as a Substance Abuse Counselor, Fetal Alcohol Spectrum Disorder trainer, and Intoxicated Driver Program Assessor certified by the State of Wisconsin. She also serves as an adjunct member of the faculty at Concordia University, UW-Parkside, and Gateway Technical College.
A recording of the presentation and a certificate of attendance will be available 24-48 hours after completion.
Click Here to Watch the Webinar
ToxTime: Poster Overview – Prenatal Exposure to Kratom
Please join us for ToxTime with Amy Racines, Research and Development Projects Coordinator at USDTL, for a brief scientific poster overview presentation discussing kratom exposure and detection in newborn umbilical cord tissue.
Amy Racines is the Research and Development Projects Coordinator at USDTL, where she develops and validates new extraction, Immunoassay, LDTD/MS/MS, GC/MS, and LC/MS/MS methods. She holds a Master’s degree in Forensic Science from the University of Florida and has been with UDSTL for over a decade. Amy has papers published in scientific journals related to umbilical cord research and Mass Spectrometry and is a member of many forensic and science-related organizations, including the position of previous President of the Midwest Association of Toxicology and the Therapeutic Drug Monitoring (MATT) and Chicago Chromatography Discussion Group (CCDG).
A recording of the presentation and a certificate of attendance will be available 24-48 hours after completion.
Click Here to Watch the Webinar
By: Amy Racines, MS, Research & Development Senior Project Coordinator
Psychedelics are a subclass of hallucinogens that produce changes in perception, mood, and cognitive processes. The most popular psychedelics include lysergic acid diethylamide (LSD), psilocybin, mescaline, and dimethyltryptamine (DMT).
Where Do They Come From
Psilocybin and mescaline are naturally occurring and produced from fungi and the Mexican peyote cactus, respectively.1 LSD, on the other hand, is chemically synthesized. DMT can be chemically synthesized, but most commonly is extracted from a variety of different plants.

Mexican peyote cactus | Sourced by Freepik©Stock
Usage Over Time
Psychedelic use dates back as early as 4000 BC, with evidence of psilocybin and mescaline being used in religious ceremonies.2 DMT was first synthesized in 1931, while LSD was first synthesized in 1943. Both LSD and DMT gained popularity in the 1960s and then in the early 1970s were classified as Schedule 1 drugs.3 Mescaline and psilocybin followed suit and were classified as Schedule 1 drugs in 1971.
After the psychedelics became scheduled, there appeared to be a decrease in usage, but more recently psychedelic use has been on the rise. LSD use rose from 0.55% in 2015 to 0.86% in 2018.4 While overall usage of LSD is still low, that was a 56 percent increase in usage over just 3 years. Psilocybin use has also been on the rise: 8.5% of adults reported usage in 2016, while 9.6% of adults reported usage in 2018.5 Less is known about DMT and mescaline trends, though one study reports mescaline usage has decreased from 2002-2019.6
Getting More Mainstream
We may expect to see a further increase in psychedelic usage due to the increasing popularity of microdosing.7 Microdosing is periodically ingesting minute quantities of psychedelic drugs as a performance-enhancing activity. The levels of psychedelics consumed are so low that a hallucinogenic effect is not experienced, but users report feeling improved mood and focus. There is no scientific literature supporting or refuting the effects of microdosing.

Psilocybin mushrooms, commonly known as magic mushrooms | Sourced by Freepik©Stock
The increased usage of psychedelics is accompanied with mainstream media on the subject. Hulu released a limited series entitled Nine Little Strangers in which the main character, a host at a luxurious wellness retreat in California, microdoses her guests without their knowledge or consent. The creator of the series was reported as stating that he hopes the series will help these types of therapies go mainstream .8 Similarly, Netflix released a movie entitled Have a Nice Trip in which celebrities reminisce about the experiences they had while under the influence of psychedelics. The movie normalizes and makes light of psychedelic usage while failing to mention any of the dangers or negative effects the users may experience. Additionally, just like with marijuana, retail companies have launched apparel and accessories with symbols and designs relating to psychedelics.
Currently, psychedelics are still illegal, but that may soon change. Psilocybin is currently being researched and may receive FDA clearance for the treatment of depression.9 Experts predict the FDA may approve the therapeutic use of psilocybin and MDMA (for PTSD) in as little as 1-2 years. This possible shift in legislation has the potential to change many aspects of the pharmaceutical and drug industry.
References:
- https://www.sciencedirect.com/topics/biochemistry-genetics-and-molecular-biology/mescaline#:~:text=Mescaline%2C%20which%20is%20derived%20from,to%20psilocin%2C%20the%20active%20moiety.
- https://www.visualcapitalist.com/sp/the-history-of-psychedelics-part-1-of-2/
- https://www.deadiversion.usdoj.gov/drug_chem_info/dmt.pdf
- https://filtermag.org/lsd-increase-research/
- https://akjournals.com/view/journals/2054/5/1/article-p17.xml
- https://www.sciencedirect.com/science/article/pii/S2352853222000499
- https://www.ncbi.nlm.nih.gov/pmc/articles/PMC6600464/
- https://www.latimes.com/entertainment-arts/tv/story/2021-09-15/nine-perfect-strangers-hulu-psychedelic-psychoactive-jonathan-levine
- https://www.nytimes.com/2022/10/25/health/psychedelic-drug-therapy-patents.html
Sign up here to learn more and receive our newsletter on the latest updates with USDTL.
ToxTime: Ethyl Glucuronide (EtG) in Hair and Nail – A review and Recent Updates
Please join us for ToxTime with Joseph Jones, Ph.D., NRCC-TC, Chief Operating Officer at USDTL, as he presents on what is new with using hair and nail to detect Ethyl Glucuronide (EtG), a long-term ethanol biomarker.
What You’ll Learn
- What is Ethyl Glucuronide (EtG)
- Ethyl Glucuronide (EtG) testing in
- Urine
- Hair
- Nail
- Umbilical Cord Tissue
- A brief overview of previous studies
- And more…
Click Here to Watch the Webinar
When drugs are swallowed, they may be broken down (metabolized) by enzymes and/or absorbed using transporters in cells found in the small intestine. Grapefruit juice can cause problems with these enzymes and transporters, causing too much or too little drug in the body.
Some drugs, like statins used to lower cholesterol, are broken down by enzymes. Grapefruit juice can block the action of these enzymes, increasing the amount of drug in the body and may cause more side effects.

Photo from the U.S. Food & Drug Administration
Other drugs, like Allegra (fexofenadine) used to treat allergies, are moved by transporters into the body’s cells. Grapefruit juice can block the action of transporters, decreasing the amount of drug in the body and may cause the drug to not work as well.
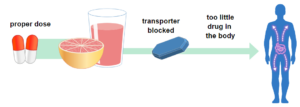
Photo from the U.S. Food & Drug Administration
Grapefruits: Food and Drug Interaction
The Canadian Medical Association Journal (CMAJ) released a review of drugs that interact with Grapefruit, “43 drugs in dangerous ways.”
List of medications that may cause severe side-effects when interacting with grapefruit.
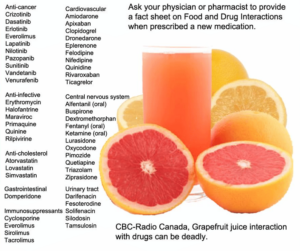
Image by CBC Radio Canada, Information from the Canadian Medical Association Journal
Information collected from:
- https://www.fda.gov/consumers/consumer-updates/grapefruit-juice-and-some-drugs-dont-mix
- https://www.cmaj.ca/content/185/4/309
- https://www.cbc.ca/news/health/grapefruit-juice-interaction-with-drugs-can-be-deadly-1.1253489
These days, having a “drink” can be deceiving. The alcohol content can vary drastically from one drink to the next.

A standard drink is any beverage that contains 14g (0.6) of pure alcohol. Amounts vary depending on the percentage of Alcohol by Volume (ABV).

Blood alcohol concentration levels for 6 drinks within 12 hours can differ greatly depending on drinking behavior and individual metabolism.

The National Institute on Alcohol Abuse and Alcoholism (NIAAA) defines binge drinking as a pattern of drinking that brings a person’s blood alcohol concentration (BAC) to 0.08 grams percent or above. This typically happens when men consume 5 or more drinks and when women consume 4 or more drinks in about 2 hours.
The Bottom Line
Self-report screening of maternal drinking during pregnancy is currently the standard test for monitoring maternal alcohol consumption and identifying alcohol-exposed newborns. However, misinformation on what defines binge drinking means self-report may not be reliable.
Alcohol biomarkers can be used as objective measurements for monitoring maternal alcohol consumption and screening for prenatal alcohol exposure.
Learn More About Alcohol Biomarker Testing
We are here to clear up some of the confusion that can surround the issue of alcohol biomarker detection and to give you the answers you need.
Contact us if you have questions or inquiries about our process or procedures. Please call 847.375.0770. Have a question but don’t want to reach out? Check out our Frequently Asked Questions (FAQs) section, where you’ll find answers to common and not-so-common questions.
By: Amy Racines, MS, Research & Development Senior Project Coordinator

Sourced by Freepik Company S.L.
Selective serotonin reuptake inhibitors (SSRIs) are a class of drugs that can be used to treat depression, anxiety, or other psychological disorders. SSRIs function by blocking the reabsorption of serotonin into neurons, causing an artificially high level of serotonin in the brain. The first SSRI, fluoxetine, was introduced into the market in 1988 as a safer alternative to tricyclic antidepressants (1). From 2015-2018, 13.2% of adults used antidepressants, and SSRIs account for approximately 70% of antidepressants prescribed (2,3).
Approximately 5.5% of pregnant women in North America used SSRIs during their pregnancy in 2019 (4). The medical opinion on the safety of taking SSRIs during pregnancy is complex. Untreated mental illness of an expecting mother can be a threat to the developing fetus, with an increased risk of preterm birth and low birth weight (5). Additionally, the babies of untreated depressed mothers can have been exposed to higher levels of cortisol, which increases the baby’s risk of developing mental illness later in life.
However, SSRI use during pregnancy might pose a risk to the developing fetus since about 30 percent of babies exposed in-utero will experience neonatal abstinence syndrome upon birth (5). Additionally, some studies have suggested SSRI use during pregnancy can be linked to an increased risk of persistent pulmonary hypertension, which is a birth defect affecting the baby’s lungs. Further studies have linked using a specific SSRI, paroxetine, during pregnancy to cardiac, brain, and abdominal birth defects (6). Still, other studies draw no link between SSRI use during pregnancy and adverse fetal outcomes. Overall, the various studies on SSRIs and their safety during pregnancy are conflicting, and more data is needed to draw more reliable conclusions.
Resources:
- https://www.ncbi.nlm.nih.gov/pmc/articles/PMC181155/
- https://www.cdc.gov/nchs/products/databriefs/db377.htm
- https://www.frontiersin.org/articles/10.3389/fpsyt.2020.00035/full
- https://www.sciencedirect.com/science/article/abs/pii/S0165032719331854
- https://www.hopkinsmedicine.org/health/wellness-and-prevention/antidepressants-and-pregnancy-tips-from-an-expert
- https://www.cdc.gov/pregnancy/meds/treatingfortwo/features/ssrisandbirthdefects.html
Sign up here to learn more and receive our newsletter on the latest updates with USDTL.
- Forensic vs. Clinical Drug Testing: Why Flexibility Matters for Your Organization
- USDTL’s Integration and Partnership With CourtFact
- New Year, New Capabilities: Offering Forensic & Clinical Testing Options
- Weather Delay
- The Detection of Delta-9-tetrahydrocannabinol, Delta-8-tetrahydrocannabinol, Delta-10-tetrahydrocannabinol, and Cannabidiol in Hair Specimens
- Umbilical Cord Tissue Testing for Ketamine
- Drugs of Abuse: A DEA Resource Guide (2024)
- Beyond THC and CBD: Understanding New Cannabinoids
- February 2026 (1)
- January 2026 (3)
- October 2025 (1)
- July 2025 (3)
- May 2025 (2)
- April 2025 (2)